Author: Anila B. Elliott, MD - University of Michigan - C.S. Mott Children’s Hospital
An infant with cyanotic heart disease experiences ongoing bleeding after initial post-bypass resuscitation with platelets and fibrinogen concentrate, so viscoelastic testing is performed. Which of the following rescue agents used for refractory post-bypass bleeding should be utilized for first-line treatment in this infant given the following viscoelastic test?

EXPLANATION
Peri-operative bleeding following pediatric cardiac surgery that involves cardiopulmonary bypass (CPB) is associated with multifactorial coagulopathy, including dilution of clotting factors, platelet dysfunction, hypothermia, and inflammatory activation. Neonates and infants are more at risk due to immature hemostatic systems and often longer bypass times due to complexity of procedure1,2.
Historically, fresh frozen plasma was the primary option for factor replacement during cardiac surgery. However, due to the risks of traditional transfusions, there has been off-label usage of factor concentrates, especially in this high-risk population, since the early 2000s1. Initially developed for hemophilia patients in the 1970s and 1980s, factor concentrates are now increasingly utilized in cardiac surgery due to rapid reconstitution, reduced transfusion risks such as infection, fluid overload, or transfusion reactions, as well as efficacy in correcting specific deficiencies1.
Despite these advantages, these agents have a risk of thrombosis, which can be higher with activated factor products2,3. Surgery and exposure to the CPB circuit and blood products triggers systemic inflammation, which activates the coagulation cascade, sometimes overwhelming natural anticoagulants, such as anti-thrombin. Pediatric patients, especially neonates and infants, naturally have immature and variable levels of coagulation factors, making them more vulnerable to shifts toward hypercoagulability post-operatively. The perioperative administration of platelets, plasma, and procoagulant agents combined with reduced natural anticoagulants during or after surgery can tip the balance toward thrombosis1,2,4.
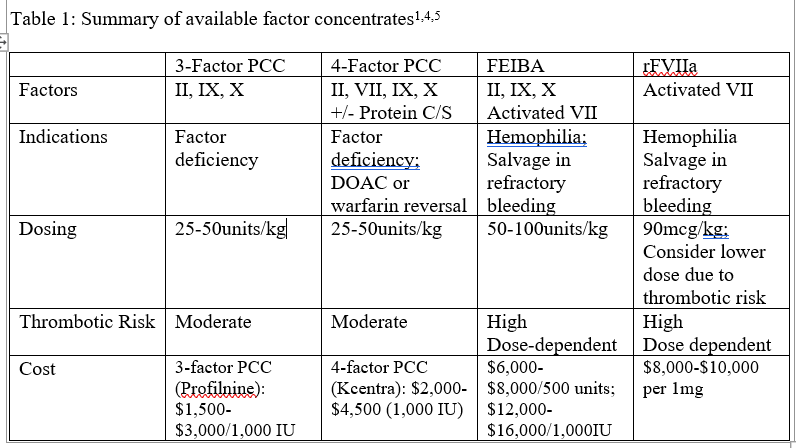
4-factor prothrombin complex concentrate (PCC; Kcentra) contains factors II, VII, IX, and X. It is recommended in European and US guidelines for perioperative coagulopathy with a moderate thrombotic risk. Due to the lack of factor VII in 3-factor PCC, it is typically less effective in normalizing INR. Factor eight bypass activity (FEIBA) and recombinant factor VIIa (NovoSeven) may be indicated in refractory cases but have been associated with higher thrombosis rates3. Recent studies suggest that 4-factor PCC may be safer than recombinant factor VIIa, with similar efficacy and lower risk of thrombosis in post-CPB bleeding3,5.
In the above EXTEM, there is a prolonged clotting time, low amplitude at all time points, and low maximum clot firmness indicating a delayed initiation of clot formation and poor clot strength, consistent with deficiency of coagulation factors, platelet dysfunction and likely fibrinogen levels. Assuming the other components (platelets and fibrinogen) have been replaced, 4-factor PCC, choice B, would be the best choice from a cost, safety and efficacy standpoint.
PCCs were first used to replenish factor IX in patients with hemophilia A and B, especially in those with inhibitors to factor VIII1. Dosing is therefore based on the amount of factor IX present in these factor concentrates. See table 1 for a summary of the various concentrates available for off-label use for post-CPB bleeding.
REFERENCES
1. Guzzetta, NA., Williams, GD. Current use of factor concentrates in pediatric cardiac anesthesia. Paediatr Anaesth 2017; 27(7):678-687
2. Navaratnam, M., Mendoza, JM., Zhang, S., et al. Activated 4-factor Prothrombin complex concentrate as a hemostatic adjunct for neonatal cardiac surgery: a propensity score-matched cohort study. Anesth Analg 2023; 136(3):473-482
3. Faraoni, D., Guindi, A., Ankola, AA., et al. Retrospective comparison of recombinant activated factor VII versus 4-factor prothrombin complex concentrate in cardiac surgery patients. J Cardiothorac Vasc Anesth 2024; 38(2):388-393
4. Casselman, FPA., Lance, MD., Ahmed, A., et al. 2024 EACTS/EACTAIC Guidelines on patient blood management in adult cardiac surgery in collaboration with EBCP. European Journal of Cardio-thoracic Surgery 2025; 67(5): ezae352
5. Budd, AN., Parulkar, SD., Carabini, LM., et al. 4-factor prothrombin complex concentrates and factor VIII inhibitor bypass activity use in cardiac surgery. Blood Coagulation & Fibrinolysis 2025; 36(1):18-25