June 2026 ECHO Question of the Month Author:
David Preston, DO
Assistant Professor, Department of Anesthesiology
UT Southwestern Medical Center
Children’s Health, Dallas
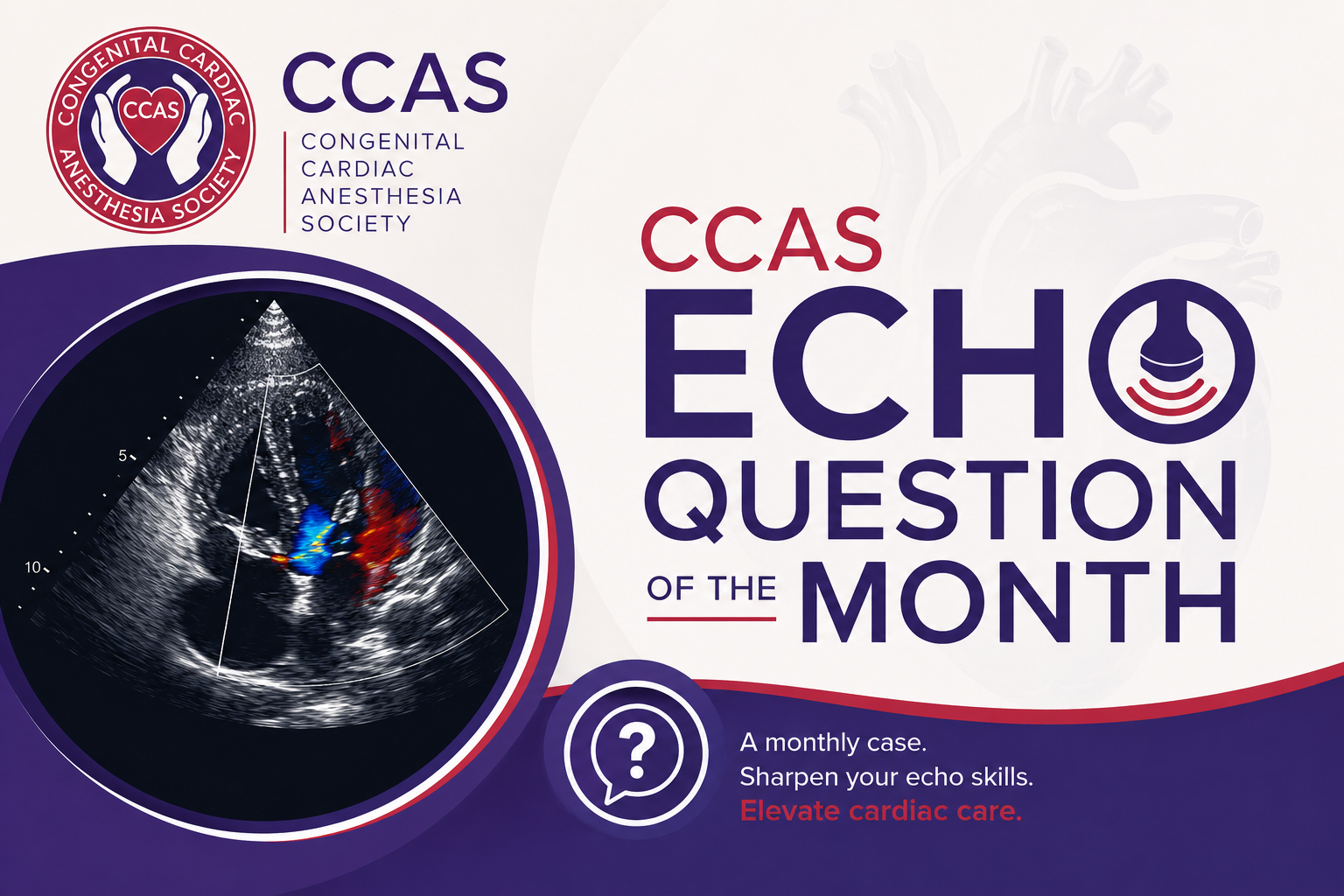
A 17-year-old male with a history of a bicuspid aortic valve resulting in mixed aortic stenosis (AS) and aortic insufficiency (AI) and a dilated aortic root presents for a Ross procedure. His pre-operative TEE exam revealed the following images:
Image 1
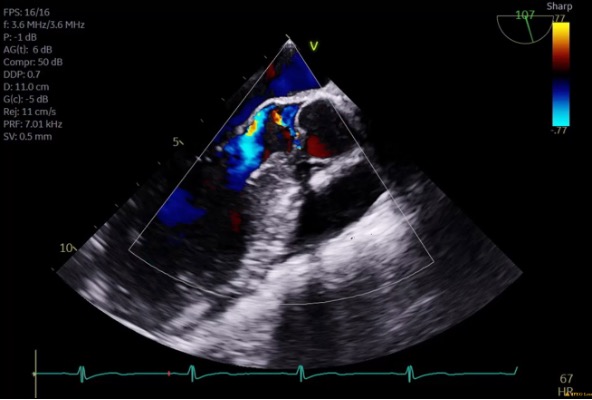
Image 2

Image 3
Answer
Image 1 is a mid-esophageal long axis view, typically found at an omniplane angle of 120 degrees. Image 2 is a mid-esophageal aortic valve short axis view, typically found at an omniplane angle between 30 and 60 degrees.
Question 2
The mean gradient measured across the aortic valve is 17mmHg. Based on this, what is the severity of aortic stenosis?
Answer
A mean gradient of 17mmHg indicates mild stenosis. When using gradients to determine severity of aortic stenosis, <20mmHg indicates mild stenosis, 20-40mmHg indicates moderate stenosis, and >40mmHg indicates severe stenosis.
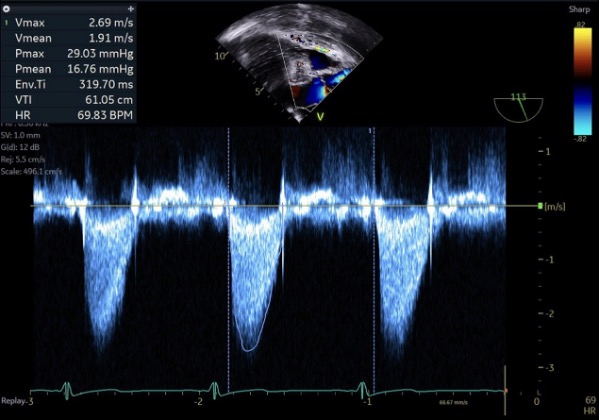
The patient’s pre-bypass course and repair are uneventful. The TEE after separating from cardiopulmonary bypass shows the following:
Image 4
Answer
The residual lesion present is aortic regurgitation. The right-side panel of Image 4 shows a color doppler pattern of blood flow back across the aortic valve into the left ventricle during diastole.
Question 4
How would you describe the jet? What does this mean and what would be the best way of measuring the severity of this valvular lesion?
Answer
This regurgitant jet would be best described as eccentric. Eccentric aortic regurgitation, in contrast with central aortic regurgitation, is a pattern in which the regurgitant jet does not flow centrally through the aortic valve into the left ventricle, but at an angle. This angular trajectory may be due to either coaptation geometry (especially in the setting of a bicuspid aortic valve), or defects in the valve leaflets themselves. The evaluation of aortic regurgitation in the setting of an eccentric jet may not allow for accurate qualitative or semiquantitative measures of regurgitation which includes jet density or jet width in the left ventricular outflow tract (vena contracta). Less direct measures such as pressure half-time and diastolic flow reversal in the descending aorta may be necessary.
The decision is made to attempt to repair the neo-aortic insufficiency via commissuroplasty of the neo-aortic valve. TEE images following this repair reveal the following:
Image 5
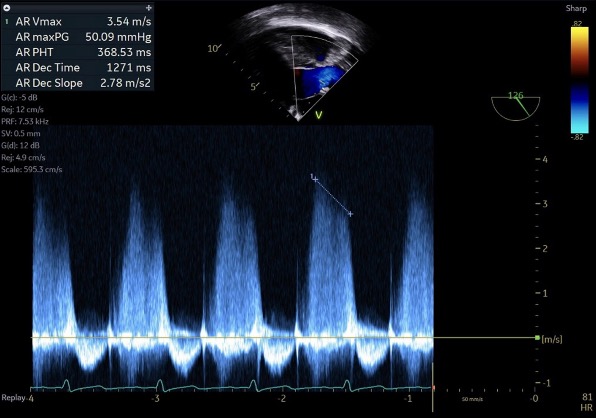
Image 6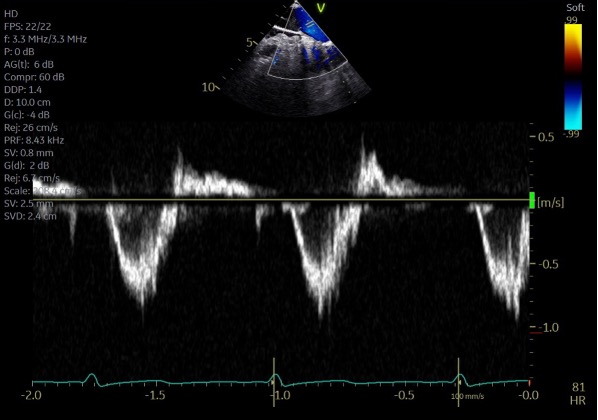
Question 5
Based on the pressure half time of 368ms in Image 6, what is the severity of the residual aortic regurgitation?
Answer
A pressure half-time (PHT) of 368ms indicates moderate aortic regurgitation. Pressure half time is a measure of the speed of equalization of pressures between aortic and left ventricular pressures in diastole. More specifically, PHT is the time it takes for the pressure gradient between the aorta and left ventricle to reach half its original value. More regurgitation allows for more rapid equalization of these pressures. PHT values for mild regurgitation are >500ms, moderate regurgitation are 500-200ms, and severe regurgitation are <200ms.
Answer
Image 6 shows a pulse-wave doppler profile in the descending thoracic aorta (DTA). The prominent negative deflection on the Y axis during systole indicates blood flow down the DTA, away from the TEE probe, during systole. However, the small positive deflection on the Y axis during diastole indicates blood flowing back toward the TEE probe during diastole as regurgitant blood flows back across the aortic valve. The more prominent and consistent this deflection, the more severe the regurgitation. The term holodiastolic flow reversal means there is reversal of blood flow (i.e. a positive deflection on a pulse-wave doppler profile) throughout the entirety of diastole, which indicates severe regurgitation. Because holodiastolic flow reversal was present, but the PHT was only 368, the regurgitation was classified as moderate to severe.
Due to the persistence of aortic regurgitation, the decision is made to proceed with a Bentall procedure (Aortic valve, aortic root and ascending aorta replacement). TEE images after this repair reveal the following:
Image 7
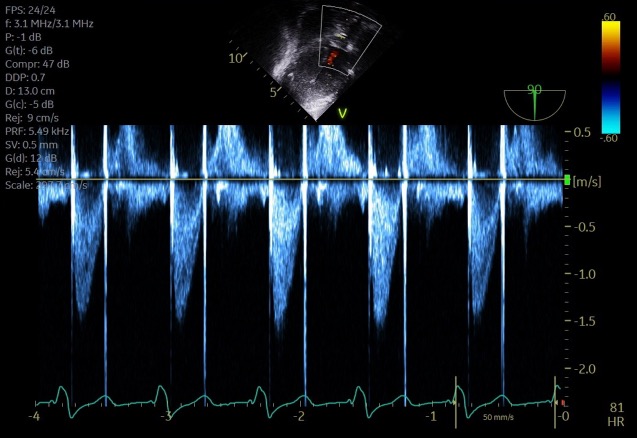
Question 7
What is the significance of the bright vertical lines visualized on either side of this continuous wave doppler profile?
Answer
This image shows a continuous wave doppler (CWD) profile of blood flow across the aortic valve in the deep transgastric view. The flow is depicted as a negative deflection on the Y axis because the flow is travelling away from the TEE probe resulting in a negative doppler shift. Each peak is a visualization of instantaneous velocities of blood flow over time, in this case across the aortic valve. A typical CWD profile does not include the bright vertical lines visualized at both the beginning and end of systole in each cardiac cycle in Image 7. These lines are a normal artifact created by the opening and closing of this patient’s new mechanical aortic valve and are pathognomonic for the presence of a mechanical prosthesis.
Clinical Note
The Ross procedure was first introduced in 1967 by Donald Ross, in which a diseased aortic valve is replaced with a pulmonary autograft in the aortic position and a pulmonary allograft in the pulmonic position. Recently, the Ross procedure has increased in popularity secondary to promising long term survival and quality of life outcomes compared to mechanical or bioprosthetic aortic valve replacement in the setting of appropriate patient selection at experienced centers.
The Ross procedure is particularly favorable for younger patients with stenosis as their primary pathology who would benefit from more favorable long term valvular dynamics compared to bioprosthetic valves as well as freedom from the lifelong systemic anticoagulation mandated by a mechanical valve. Connective tissue disorders, multi-vessel coronary artery disease, and a dysfunctional pulmonary valve are contraindications to the procedure. Pre-operative evaluation should include CT angiography and echocardiography, with special attention to coronary anatomy and confirmation of a functional and tri-leaflet pulmonic valve that is appropriately sized for placement in the aortic position. Modifications to the Ross procedure include placement of a Dacron graft around the pulmonary autograft to prevent excessive root dilatation, as well as aortic root enlargement to accommodate a larger pulmonary autograft. Post-bypass, the pulmonary autograft should display a hemodynamic profile similar to a normally functioning aortic valve without a significant gradient. Pre-existing fenestrations in the pulmonary autograft leaflets may be unmasked by exposure to systemic pressures and should be addressed if the resultant regurgitation is severe. Early post-operative complications may include autograft dysfunction, arrhythmia, complications related to coronary re-implantation, and bleeding. Long term complications may include regurgitation, stenosis, or annular dilatation of the autograft, along with dysfunction of the pulmonary allograft.
Recent studies have demonstrated freedom from re-intervention rates of 80% and survival rates of 80-90% at 20 years. In the setting of re-intervention, transcatheter aortic valve interventions have been used for failing autografts but require further investigation before regular use. Transcatheter options are routinely employed for pulmonary allograft dysfunction if coronary anatomy is favorable.
References
- Bloom JP, Nam L, Sá MP, Williams E, Ouzounian M, El-Hamamsy I, Hopkins W, Yeh DD. Ross Procedure Renaissance: A Contemporary Review of Patient Selection, Technique, and Long-Term Outcomes in Adults. J Am Heart Assoc. 2026 Jan 6;15(1):e044454. doi: 10.1161/JAHA.125.044454.
- Galzerano D, Kholaif N, Al Amro B, Al Admawi M, Eltayeb A, Alshammari A, Di Salvo G, Al-Halees ZY. The Ross Procedure: Imaging, Outcomes and Future Directions in Aortic Valve Replacement. J Clin Med. 2024 Jan 22;13(2):630. doi: 10.3390/jcm13020630. PMID: 38276135; PMCID: PMC10816914.
- Laurin C, Notenboom ML, Chen L, Williams EE, El-Hamamsy I. The Ross Procedure in Adults. Journal of the Heart Valve Society. 2024;1(1). doi:1177/30494826241296678
- Mathew JP, Swaminathan M, Ayoub CM, eds. Clinical Manual and Review of Transesophageal Echocardiography. 3rd McGraw-Hill Education; 2019