Author: Anila B. Elliott, MD - University of Michigan - C.S. Mott Children’s Hospital
An 8-month-old infant has a history of critical aortic stenosis and endofibroelastosis complicated by need for Berlin Heart EXCOR placement at 2 months of age. They have type O blood and have been listed 1A for transplantation for months. Due to the limited pool of compatible organs, the heart failure team recommends proceeding with an ABO-incompatible heart transplant. Which of the following best explains why ABO-incompatible transplantation is feasible in this patient?
EXPLANATION
ABO-incompatible transplantation has transformed the management of the congenital cardiac patient population, where it has improved waitlist outcomes and reduced mortality, especially among infants with type O blood1,2. Multicenter studies over the past two decades have shown that ABO-incompatible heart transplantation in infants has survival, graft rejection, graft vasculopathy, and malignancy rates comparable to ABO-compatible transplantations2,3,4. Comparable success has been achieved with other solid organ and hematopoietic stem-cell transplants when isohemaglutinin titers are sufficiently low3. Recent data from the International Society for Heart and Lung Transplantation Registry showed an increase in ABO-incompatible transplants of 40% across 93 centers from 2010-20181.
Infants have immature immune systems and do not produce a significant amount of isohemaglutinins, which are antibodies that target ABO-blood group antigens. These antibodies typically emerge after exposure to environmental antigens in the first few months of life and usually remain at very low levels until about 12-24 months of age2,3,4. As a result, this immunologic immaturity has allowed for successful transplantation of organs from ABO-incompatible donors without experiencing the hyperacute rejection seen in sensitized older children and adults. The absence of the anti-A and anti-B antibodies helps prevent complement-mediated injury, which accelerates thrombosis of graft vasculature, and contributes to hemolysis during and following transplantation3. Therefore, answer choice B, infants do not produce significant isohemaglutinins against A and B antigens, is the correct answer.
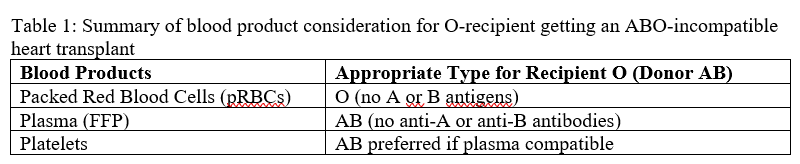
Success of this approach involves significant multidisciplinary collaboration among perioperative teams. Pre-operative plasmapheresis or intra-operative immunoadsorption may be utilized to decrease isohemagglutinin titers5. Plasma exchange is not necessary during surgery if isohemagglutinin levels are less than 1:4 to 1:164. The perfusionist therefore plays an integral role in management intra-operatively. Protocols include washing packed red blood cells (pRBCs) and plasma while ideally matching donor/recipient blood products. The cardiopulmonary bypass circuit is primed with recipient-compatible pRBCs and plasma/platelets that are free from anti-A and anti-B antibodies. During the procedure, transfusion management aims to minimize exposure to antibodies; only washed red blood cells are returned to the patient, minimizing or modifying the use of pump suckers and cell saver to avoid reintroducing antibody-rich plasma. Ultrafiltration is used to reduce antibody titers and manage fluid overload, especially in smaller patients5. Table 1 summarizes blood product considerations for a blood-type O transplant recipient.
Intra-operatively and post-operatively, monitoring for hemolysis and acute complement-mediated rejection is important. Signs of hemolysis include dark urine, elevated LDH, elevated bilirubin and declining haptoglobin. Other signs of acute rejection include hemodynamic instability and poor graft function. Other contributors to poor graft function include ischemic time, comorbidities, early infection, and suboptimal immunosuppression2,4. These patients may need increased immunosuppression due to their increased risk profile and should be closely monitored throughout the peri-operative period.
REFERENCES
1. Ungerman E, Hunter OC, Jayaraman AL, et al. The Year in Cardiothoracic Transplant Anesthesia: Selected Highlights From 2022 Part II: Cardiac Transplantation. J Cardiothorac Vasc Anesth. 2025;39(2):364-397. doi:10.1053/j.jvca.2024.10.026
2. Bansal N, West LJ, Simmonds J, Urschel S. ABO-incompatible heart transplantation-evolution of a revolution. J Heart Lung Transplant. 2024;43(9):1514-1520. doi:10.1016/j.healun.2024.03.019
3. West LJ, Pollock-Barziv SM, Dipchand AI, et al. ABO-incompatible heart transplantation in infants. N Engl J Med. 2001;344(11):793-800. doi:10.1056/NEJM200103153441102
4. Urschel S, West LJ. ABO-incompatible heart transplantation. Curr Opin Pediatr. 2016;28(5):613-619. doi:10.1097/MOP.0000000000000398
5. Foreman C, Gruenwald C, West L. ABO-incompatible heart transplantation: a perfusion strategy. Perfusion. 2004;19(1):69-72. doi:10.1191/0267659104pf708oa