Question of the Week 588
Author: Kaitlin M. Flannery, MD, MPH - Stanford University
A 7-day-old, 3.2 kg neonate presents to the emergency department with poor feeding and lethargy. Echocardiogram demonstrates previously undiagnosed hypoplastic left heart syndrome (HLHS) with mitral and aortic atresia (MA/AA), an intact atrial septum, preserved single ventricle function, and SaO2 ~ 80%. Chest radiograph shows only mild pulmonary vascular congestion without pulmonary edema. Which of the following BEST explains the absence of severe respiratory failure in this patient?
EXPLANATION
With widespread prenatal screening, most fetuses with hypoplastic left heart syndrome (HLHS) are diagnosed in utero. In patients with post-natal diagnosis, symptoms typically develop during the first few days of life as closure of the patent ductus arteriosus results in inadequate systemic blood flow and cardiovascular collapse.
A subset of patients with HLHS, approximately 6%, have an intact or highly restrictive atrial septum (IAS). These neonates often develop severe respiratory failure within minutes to hours after birth. Following delivery, pulmonary venous blood is unable to exit the left atrium (LA), resulting in profound pulmonary venous hypertension, pulmonary edema, and severe hypoxemia. Elevated LA pressure during fetal life also leads to abnormal pulmonary vascular and lymphatic development, contributing to poor outcomes despite postnatal intervention.1
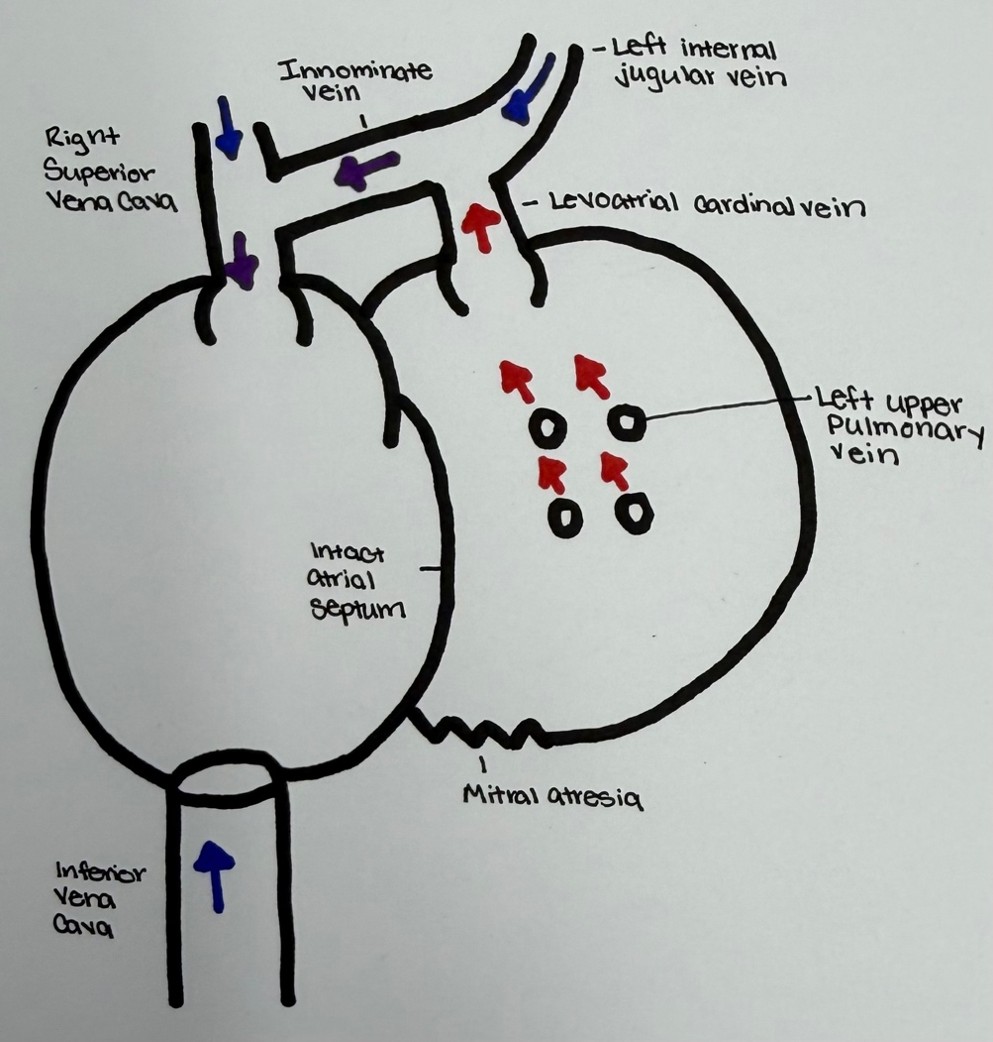
Rarely, a large, unobstructed decompressing levoatrial cardinal vein (LACV) (also commonly referred to as a levocardinal atrial vein or decompressing levocardinal vein) provides an alternative pathway for pulmonary venous drainage. The LACV is an embryologic connection between the LA and the systemic venous circulation, most commonly the innominate vein or superior vena cava. In the setting of LA outflow obstruction, this vessel can decompress the LA and pulmonary veins reducing pulmonary venous hypertension and limiting pulmonary edema despite the presence of an intact atrial septum. Consequently, affected neonates may initially appear less symptomatic than expected. However, because the LACV can become obstructed either in utero or after birth, urgent decompression of the LA through atrial septal intervention remains indicated.1
Historically, outcomes for patients with HLHS and IAS have been poor. A retrospective review from The Children’s Hospital of Philadelphia reported a 67% (12/18) 30-day mortality rate following Norwood procedure. Of the six patients who survived the Norwood procedure, three subsequently died after bidirectional Glenn procedure leaving only 17% reaching Fontan completion. Notably, all patients who survived to the Glenn stage had an unobstructed decompressing LACV.1
More contemporary outcomes have improved. A single-center retrospective review from The University of Michigan reported approximately 40% survival to Fontan completion. This improvement is driven by an aggressive multidisciplinary strategy that included fetal intervention (balloon atrial septectomy or atrial stent) when technically feasible and emergency hybrid stage 1 palliation performed immediately after birth as an IMPACT (immediate post-partum access to cardiac therapy) procedure.2
In the above scenario, the presence of an unobstructed LACV provides decompression for the left atrium, thus preventing severe pulmonary edema and respiratory distress. Increased pulmonary vascular resistance might limit pulmonary blood flow but with no egress from the left atrium, pulmonary edema would eventually develop. The presence of a ventricular septal defect would not contribute to LA decompression.
REFERENCES
1. Rychik J, Rome JJ, Collins MH, DeCampli WM, Spray TL. The hypoplastic left heart syndrome with intact atrial septum: atrial morphology, pulmonary vascular histopathology and outcome. J Am Coll Cardiol. 1999 Aug;34(2):554-60.
2. Sood V, Zampi JD, Romano JC. Hypoplastic left heart syndrome with an intact atrial septum. JTCVS Open. 2020 Apri 6:1:51-6.