Author: Kanwarpal S. Bakshi, MD – Children’s Hospital Los Angeles
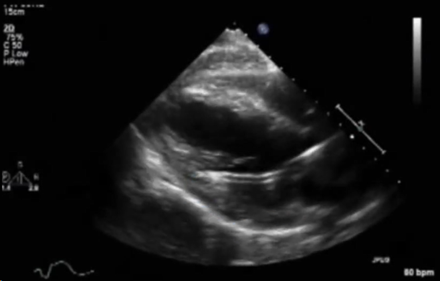
A 16-year-old female with fulminant viral myocarditis on peripheral veno-arterial (VA) ECMO support develops pulmonary hemorrhage. An Impella CP® device was inserted for left ventricular unloading while still on ECMO. A transthoracic echocardiogram was performed to confirm the position of the Impella due to concern for poor unloading. Based on the echocardiographic image below, what is the BEST next step in management?
EXPLANATION
The Impella device (Abiomed, Danvers, MA, USA) is a percutaneous microaxial flow pump that provides temporary mechanical circulatory support by actively unloading the left ventricle (LV) and maintaining systemic perfusion. It is commonly used in patients with severe heart failure, cardiogenic shock, or those undergoing high-risk coronary procedures.¹ Available devices vary by flow capacity and insertion approach, including the Impella 2.5 and CP (percutaneous, providing up to ~3.5 L/min of flow), the Impella 5.0 and 5.5 (surgically implanted with higher flow rates), and the Impella RP for right ventricular support.¹
Impella positioning is critical for its proper function and safety. For all left-sided Impella devices, the inlet must be positioned in the mid-left ventricular cavity, while the outlet should be placed in the ascending aorta.² The correct positioning can be confirmed using transesophageal echocardiography (TEE) or transthoracic echocardiography (TTE). Ideal views typically include the transgastric long axis, midesophageal long axis (TEE) or parasternal long axis (TTE) views.
On imaging, the Impella catheter appears as a bright linear echogenic structure crossing the aortic valve. The inlet is typically visualized just apical to the mitral valve plane and often displays a “teardrop sign”—an echolucent space representing blood being drawn into the pump.² The outlet should be in the proximal ascending aorta, not retracting into the valve or extending excessively. The pigtail tip (for Impella 2.5 and CP), visible as a curled loop extending toward the apex, helps reduce myocardial trauma and aids device orientation. Color doppler may reveal continuous flow from the LV to the aorta through the device when the device is properly placed and functioning. Figure 1 shows an example of incorrect positioning, as the inlet is located in the LV myocardium, while Figure 2 demonstrates the correct positioning of the Impella. The inlet positioning should be approximately 3.5–4 cm from the aortic annulus for Impella CP and 5.0, and 5 cm from the aortic annulus for the Imeplla 5.5.²
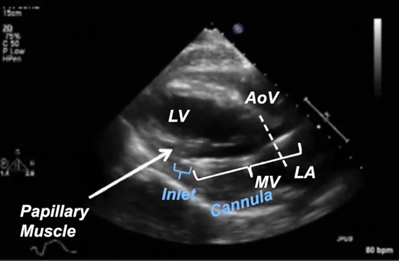
Figure 1: Improper Impella Placement. This figure shows the impella is advanced too far into the LV cavity, which can cause obstruction to blood flow in the inlet of the impella device.
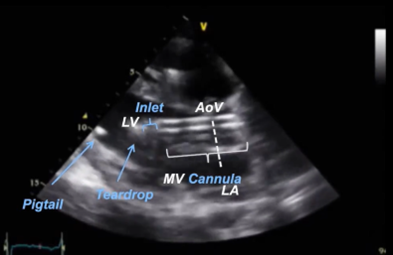 Figure 2: Proper Impella Placement. This figure shows correct placement of the impella device, with the inlet in the mid LV cavity approximately 3.5cm from the aortic valve annulus.
Figure 2: Proper Impella Placement. This figure shows correct placement of the impella device, with the inlet in the mid LV cavity approximately 3.5cm from the aortic valve annulus.
In the setting of VA ECMO, afterload increases due to retrograde aortic flow, especially when inserted peripherally.4 If LV function is severely impaired, this can result in LV distention, stasis, pulmonary hemorrhage, and delayed myocardial recovery. The addition of an Impella device to VA-ECMO (also known as ECPella) provides active LV unloading and improves pulmonary venous drainage, reducing left atrial pressure and preventing complications such as pulmonary edema and hemorrhage.³ In addition, LV unloading with an Impella is associated with lower mortality in patients with cardiogenic shock supported with VA-ECMO.³ An alternative approach to mechanical LV decompression is atrial septostomy, which creates a left-to-right atrial shunt to reduce left atrial pressure, as well as venting through the aorta or pulmonary vessels.4
Option B (advance Impella further into the LV) is incorrect because the device is already too deep. Advancing it could lead to entrapment or damage. Option C (increase ECMO RPM) may increase afterload and exacerbate LV distension.
REFERENCES
1. Zein R, Patel C, Mercado-Alamo A, Schreiber T, Kaki A. A Review of the Impella Devices. Interv Cardiol. 2022;17:e05. Published 2022 Apr 8. doi:10.15420/icr.2021.11
2. Abiomed. Using echocardiography for Impella positioning. HeartRecovery.com. Accessed August 21, 2025. https://www.heartrecovery.com/en-us/education/education-library/echo-for-impella-how-to-measure-and-determine-proper-position
3. Meani P, Lorusso R, Pappalardo F. ECPella: Concept, Physiology and Clinical Applications. J Cardiothorac Vasc Anesth. 2022;36(2):557-566. doi:10.1053/j.jvca.2021.01.056
4. AlGhamdi M, Saiydoun G, Lebreton G, Mazzucotelli JP. Percutaneous atrial septostomy for left ventricular unloading in patients on peripheral venoarterial extracorporeal membrane oxygenation: A systematic review and meta-analysis. Am Heart J Plus. 2025;54:100542. Published 2025 Apr 9. doi:10.1016/j.ahjo.2025.100542