Author: Michael A. Evans, MD; Ann & Robert H. Lurie Children’s Hospital of Chicago, Northwestern Feinberg School of Medicine
A 25-year-old woman with a history of hypoplastic left heart syndrome status-post Fontan palliation presents at 35-weeks gestation in active labor after spontaneous rupture of membranes. Which of the following complications is MOST LIKELY to occur in a parturient with single ventricle physiology intrapartum or postpartum?
EXPLANATION
Maternal congenital heart disease (CHD) poses a major risk to mother and child. There is a higher risk of spontaneous abortions and fetal demise in mothers with CHD when compared to the general population, a higher preterm birth rate (10-12% for all CHD), a higher frequency of adverse neonatal events (small for gestational age, respiratory distress syndrome, intraventricular hemorrhage), and a higher perinatal mortality rate (>4x higher than the general population).
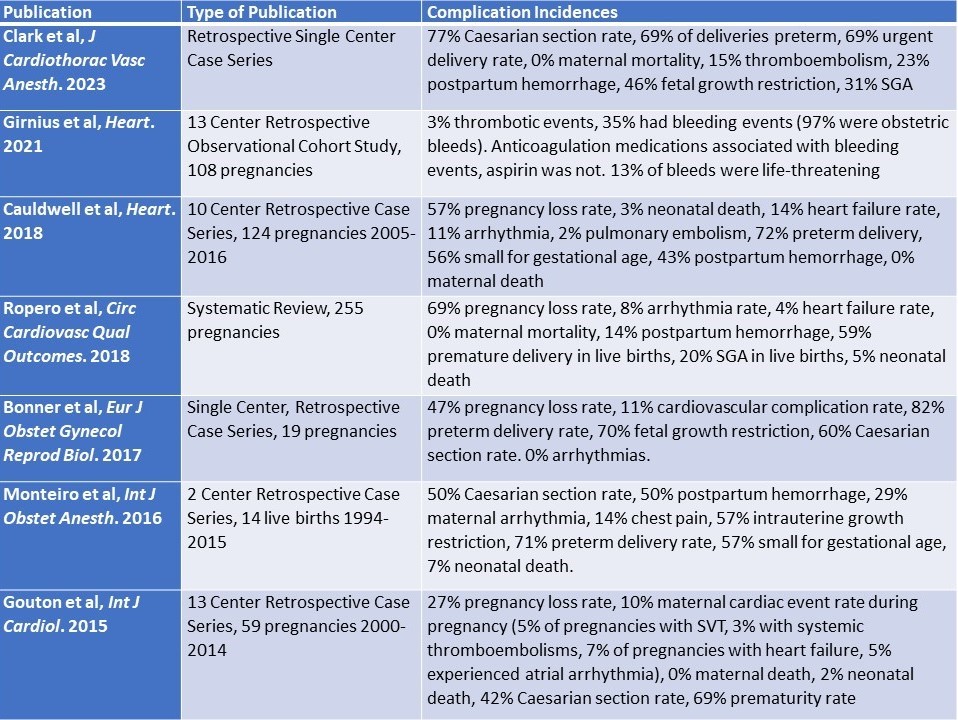
When pregnancies in mothers with Fontan physiology are examined, the adverse event rates throughout pregnancy, delivery, and postpartum are all increased when compared to other forms of CHD and in mothers without CHD. The most commonly observed complications in Fontan pregnancies and parturients include preterm delivery (59-82%), thromboembolic events (2-15%), postpartum hemorrhage or bleeding events (14-50%), fetal growth restriction (46-70%), small for gestational age (20-57%), pregnancy loss (27-69%), arrhythmia (0-29%), ventricular dysfunction or heart failure (4-14%), and neonatal death (2-7%).
The risk of preterm delivery (59-82% of Fontan pregnancies) is consistently significantly higher than any of the listed other observed complications, thus Answer D is correct. Although arrhythmias (Answer A, 0-29% of Fontan pregnancies) are more common in single ventricle mothers compared to the general population, they are not more common than preterm
deliveries. The same is true of postpartum hemorrhage (Answer B, 14-50%) and thromboembolic events (Answer C, 2-15%), which are both clinically important and contribute significantly to maternal morbidity in Fontan pregnancies.
A summary of selected literature examining mothers with Fontan physiology and perinatal outcomes can be found below:
REFERENCES
Clark DE, Staudt G, Byrne RD, et al. Anesthetic Management in Parturients With Fontan Physiology. J Cardiothorac Vasc Anesth. 2023;37(1):167-176. doi:10.1053/j.jvca.2022.07.009
Girnius A, Zentner D, Valente AM, et al. Bleeding and thrombotic risk in pregnant women with Fontan physiology. Heart. 2021;107(17):1390-1397. doi:10.1136/heartjnl-2020-317397
Garcia Ropero A, Baskar S, Roos Hesselink JW, et al. Pregnancy in Women With a Fontan Circulation: A Systematic Review of the Literature. Circ Cardiovasc Qual Outcomes. 2018;11(5):e004575. doi:10.1161/CIRCOUTCOMES.117.004575
Cauldwell M, Steer PJ, Bonner S, et al. Retrospective UK multicentre study of the pregnancy outcomes of women with a Fontan repair. Heart. 2018;104(5):401-406. doi:10.1136/heartjnl-2017-311763
Canobbio MM, Warnes CA, Aboulhosn J, et al. Management of Pregnancy in Patients With Complex Congenital Heart Disease: A Scientific Statement for Healthcare Professionals From the American Heart Association. Circulation. 2017;135(8):e50-e87. doi:10.1161/CIR.0000000000000458
Bonner SJ, Asghar O, Roberts A, Vause S, Clarke B, Keavney B. Cardiovascular, obstetric and neonatal outcomes in women with previous fontan repair [published correction appears in Eur J Obstet Gynecol Reprod Biol. 2018 Jan 4;:]. Eur J Obstet Gynecol Reprod Biol. 2017;219:53-56. doi:10.1016/j.ejogrb.2017.10.013
Monteiro RS, Dob DP, Cauldwell MR, Gatzoulis MA. Anaesthetic management of parturients with univentricular congenital heart disease and the Fontan operation. Int J Obstet Anesth. 2016;28:83-91. doi:10.1016/j.ijoa.2016.08.004
Gouton M, Nizard J, Patel M, et al. Maternal and fetal outcomes of pregnancy with Fontan circulation: A multicentric observational study. Int J Cardiol. 2015;187:84-89. doi:10.1016/j.ijcard.2015.03.344
