Author: Nicholas Houska, DO and Raveendra Morchi, MD - University of Colorado, Children's Hospital Colorado
A 4-month-old male presents for surgical closure of a large ventricular septal defect (VSD) due to failure to thrive and feeding intolerance. Which of the following types of VSD is associated with the HIGHEST risk of injury to the conduction system and subsequent heart block during surgical closure?
EXPLANATION
Septation of the ventricles occurs in the first trimester and is intimately related to development of the atrioventricular canals and the outflow tracts. The muscular septum forms from an infolding of ventricular muscle which develops to align with the conal septum of the ventricular outflow tracts. The final area of septation is the membranous septum which develops from the endocardial cushions. The development of the of the atrioventricular node, His-Purkinje system, and bundle branches anatomically coincide with the development of the ventricular septum.
There are multiple systems of nomenclature in common usage to describe and classify VSDs, which has led to significant confusion in the literature and clinical practice. To provide uniformity of language and improve communication, the International Society for Nomenclature of Pediatric and Congenital Heart Disease has proposed a classification system which has been accepted by the World Health Organization into the 11th iteration of the international classification of diseases. Under this classification, VSDs are divided into four major groups with descriptors added for the various subtypes within each group. The four groups are: perimembranous central, inlet, trabecular muscular, and outlet. Of these, the perimembranous central type is the most common, comprising greater than 80% of clinically significant VSDs.
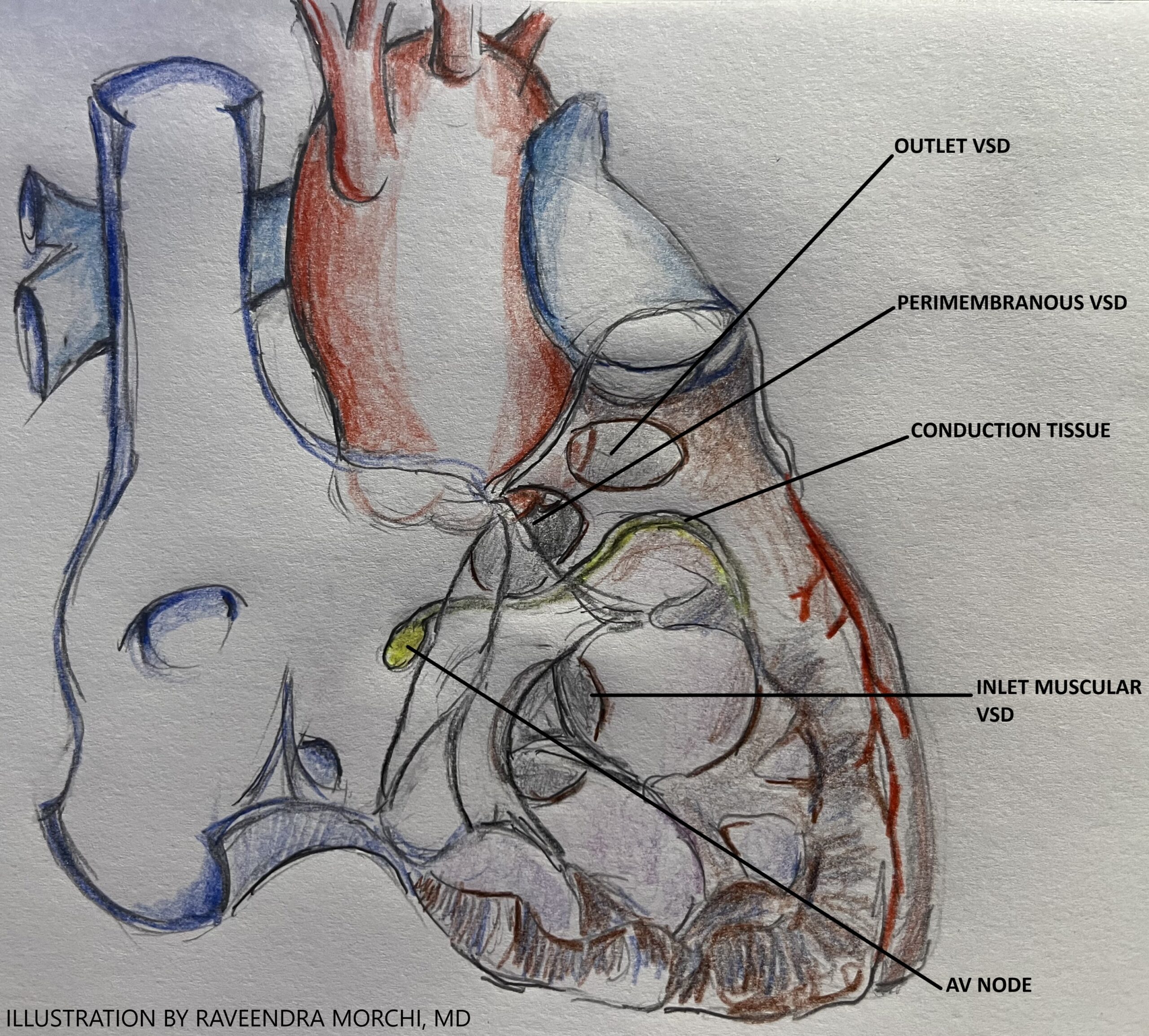
One of the most serious complications after surgical closure of a ventricular septal defect (VSD) is complete heart block, having a significant impact on long term morbidity. Perimembranous VSDs are intimately associated with the conduction system at the inferoposterior margin, namely the AV node, Bundle of His, and right bundle branch, and are at the highest risk of surgically-induced heart block (see the image below – by R. Morchi, MD, used by permission). Careful surgical technique and suture placement in this area is essential to prevent damage to the conduction system and subsequent heart block. There is also risk of perioperative heart block after closure of an inlet VSD due to close proximity to the conduction system. Trabecular muscular and outlet VSDs are located in a more remote location from the major components of the conduction system and are much less likely to result in surgical heart block after surgical closure. With improvement in surgical techniques over the years, the current incidence of complete heart block after VSD closure is less than one percent.
REFERENCES
Lopez L, Houyel L, Colan SD, et al. Classification of ventricular septal defects for the eleventh iteration of the international classification of diseases—striving for consensus: a report from the international society for nomenclature of paediatric and congenital heart disease. The Annals of Thoracic Surgery . 2018;106(5):1578-1589.
Gholampour-Dehaki M, Zareh A, Babaki S, Javadikasgari H. Conduction disorders in continuous versus interrupted suturing technique in ventricular septal defect surgical repair. Res Cardiovasc Med . 2016;5(1).
Jonas RA. Vnetricular Septal Defect. In: Comprehensive Surgical Management of Congenital Heart Disease .2nd ed. CRC Press; 2014. 331-346.
Andersen HØ, de Leval MR, Tsang VT, Elliott MJ, Anderson RH, Cook AC. Is complete heart block after surgical closure of ventricular septum defects still an issue? The Annals of Thoracic Surgery . 2006;82(3):948-956.
Lamers WH, Moorman AFM. Cardiac septation: a late contribution of the embryonic primary myocardium to heart morphogenesis. Circulation Research . 2002;91(2):93-103.
