Authors: Pedro Solorzano, MD and Destiny F. Chau, MD - Arkansas Children’s Hospital/University of Arkansas for Medical Sciences, Little Rock, AR
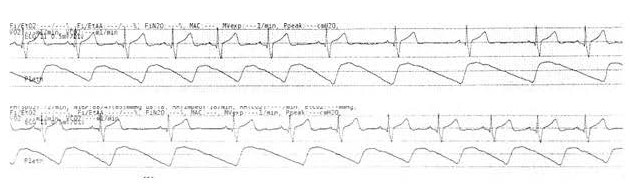
A 12-year-old boy with a history of Wolff-Parkinson-White syndrome and intermittent supraventricular tachycardia is scheduled for an electrophysiologic study. The following electrocardiographic (ECG) rhythm is noted prior to induction of anesthesia. Which of the following cardiac rhythms is MOST likely illustrated below?
EXPLANATION
Sinus arrhythmia is a variant of normal sinus rhythm (NSR) that is commonly seen in children and young adults. The heart rate increases with inspiration and decreases with expiration. This form of “respiratory sinus arrhythmia” characteristically presents with P waves of normal morphology consistent with originating from the sinus node. Each P wave is followed by a normal QRS complex, and the P-P intervals vary by more than 120 milliseconds or more than 10% of the shortest P-P interval. If the variation in rate is severe (i.e. a 100% change resulting in a heart rate of half), this is indicative of a more serious medical problem. One mechanism implicated in sinus arrhythmia involves the respiratory cycle and inherent cardiorespiratory interactions. It is postulated that inspiration inhibits vagal tone, thereby increasing the heart rate, and expiration restores the vagal tone to its previous state, such that the heart rate declines.
It is more noticeable in younger children as they have faster heart rates, and it has been seen in all children at some point during a 24-hour monitoring. Thus, in young, otherwise healthy patients without any other symptoms, sinus arrhythmia is considered a benign finding and further evaluation of sinus arrhythmia is usually unnecessary. However, severe sinus arrhythmia in older patients, often termed “non-respiratory sinus arrhythmia” in which the heart rate does not vary with the phases of respiration, may indicate underlying cardiac disease, although it is not considered a marker for structural heart disease (Issa et al).
This patient’s ECG rhythm strip shows monomorphic P waves that vary more than 10% of the shortest P-P interval. Each P-wave is followed by the patient’s baseline QRS complex (which also shows a delta wave consistent with Wolff-Parkinson-White syndrome). This is consistent with a benign form of sinus arrhythmia which requires no treatment. Atrial fibrillation typically demonstrates an irregularly irregular rhythm and P waves are not visualized. Mobitz type II is a form of second-degree heart block characterized by a constant P-P interval without lengthening of the PR interval prior to a non-conducted P wave. This type of heart block is not a normal variant and is always considered pathologic. Common causes in children include post-cardiac surgery, myocarditis, orthotopic heart transplant rejection, and post-transplant coronary artery disease.
REFERENCES
Cannon BC, Snyder CS. Disorders of cardiac rhythm and conduction. In: Shaddy R, Penny D, Feltes T, Cetta F and Mital S, eds. Moss and Adams’ Heart Disease in Infants, Children and Adolescents including the Fetus and Young Adult. 10th Edition. Philadelphia: Wolters Kluwer; 2022. 586-616.
Issa ZF, Miller JM, Zipes DP. Sinus Node Dysfunction. In: Issa ZF, Miller JM, Zipes DP, Eds. Clinical Arrhythmology and Electrophysiology. 3rd Edition. Elsevier; 2019: 238-254.