Authors: Meera Gangadharan MBBS, FAAP, FASA, University of Texas Health Science Center at Houston/Children’s Memorial Hermann Hospital AND Destiny F. Chau MD, University of Arkansas for Medical Sciences/Arkansas Children’s Hospital, Little Rock, AR
Which of the following coronary artery arrangements is MOST commonly associated with D-transposition of the great arteries?
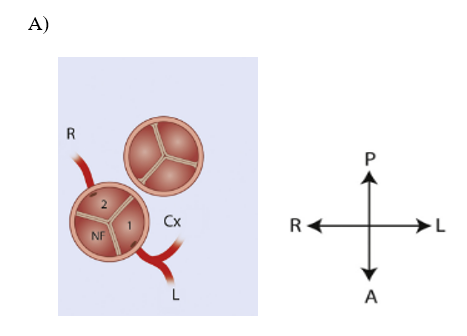
 Creative Commons Licensing from Gittenberger-de Groot et al. J Thorac Cardiovasc Surg. 2018;156(6):2260-2269
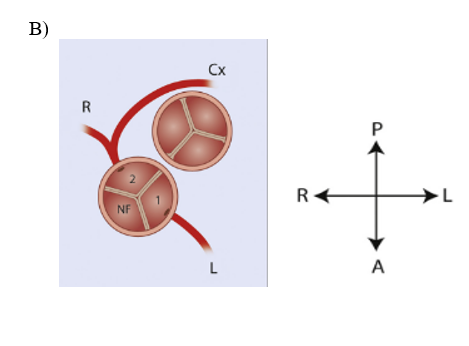
Creative Commons Licensing from Gittenberger-de Groot et al. J Thorac Cardiovasc Surg. 2018;156(6):2260-2269
EXPLANATION
Dextro transposition of the great arteries (D-TGA) is characterized by ventriculoarterial discordance and atrioventricular concordance. D-TGA comprises approximately 5% of all congenital heart lesions and is one of the most common cyanotic congenital heart diseases to present in the newborn period with an incidence of roughly 3 per 10,000 live births. The aorta arises from the morphologic right ventricle and the pulmonary artery from the morphologic left ventricle. Patients usually have levocardia, situs solitus, and D-looped ventricles. The relative position of the aortic valve to the pulmonary valve may vary. Still, the most common arrangement is the aortic valve orifice to the right and anterior to the pulmonary valve orifice. The ventricular septum may be intact or there may be a ventricular septal defect. Left ventricular outflow tract obstruction may also be present.
Coronary artery anomalies are another hallmark of transposition of the great arteries and efforts have been made to describe the coronary artery configurations in a standardized manner. Due to variations in the relative positions of the aortic and pulmonary valves to each other, the aortic valve orifice may be side-by-side, right and anterior to, or directly anterior to the pulmonary valve. The origin and subsequent course of the coronary arteries result in several different patterns. The two most common systems for describing the coronary artery configuration in D-TGA are the Yacoub classification described in 1978 and the more common Leiden Convention. The Leiden Convention was originally published in the early 1980s and was modified in 2018. It places the observer in the non-coronary cusp facing the pulmonary artery, with the right hand labeled “sinus 1” and the left hand labeled “sinus 2”. The classification then describes from which sinus each of the three major coronary arteries arise (Fig.1).
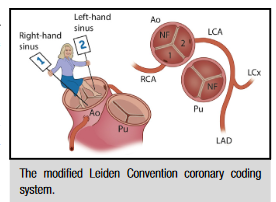 Figure 1: Illustration of Leiden nomenclature determination. [Creative Commons Licensing from Gittenberger-de Groot et al. J Thorac Cardiovasc Surg. 2018;156(6):2260-2269.]
Figure 1: Illustration of Leiden nomenclature determination. [Creative Commons Licensing from Gittenberger-de Groot et al. J Thorac Cardiovasc Surg. 2018;156(6):2260-2269.]
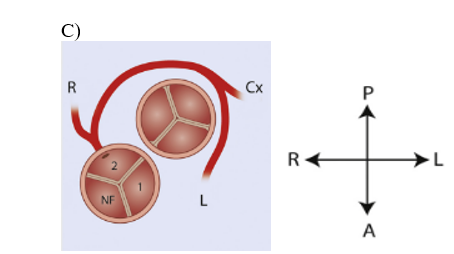
The most common surgery performed for D-TGA in the current era is the Jatene arterial switch operation (ASO). This involves transecting the pulmonary artery and aorta, a few millimeters distal to their valves and anastomosing the pulmonary artery segment to the aortic root and the aorta to the pulmonary root. The operation also requires that the coronaries be translocated to the neo-aortic (pulmonary) root. From a surgical perspective, coronary artery patterns can be grouped into three main categories: (1) the “usual” coronary pattern (70% of cases), as depicted in answer option (A), where the left and right coronaries originate from separate sinuses with the left coronary dividing into left anterior descending and circumflex branches. Coronary transfer is usually straightforward and associated with excellent outcomes; (2) coronary arteries with an anterior or posterior loop (25% of cases), in which the coronary transfer may be difficult; and (3) coronary artery pattern with a single origin or where the coronaries course between the major arterial trunks, which may be associated with an intramural segment. Coronary transfer is usually difficult and represents a high risk for morbidity and mortality. Hence a detailed description of coronary artery anatomy before surgery is critical to avoid kinking, stretching, or placing tension on the coronary arteries when they are translocated.
The most common (“usual”) coronary artery pattern present in approximately 70% of cases of D-TGA is shown in answer option A. The other two patterns are much less commonly associated with D-TGA.
REFERENCES
Gittenberger-de Groot AC, Koenraadt WMC, Bartelings MM, et al. Coding of coronary arterial origin and branching in congenital heart disease: The modified Leiden Convention. J Thorac Cardiovasc Surg. 2018;156(6):2260-2269. doi:10.1016/j.jtcvs.2018.08.009
Yacoub MH, Radley-Smith R. Anatomy of the coronary arteries in transposition of the great arteries and methods for their transfer in anatomical correction. Thorax. 1978;33(4):418-424. doi:10.1136/thx.33.4.418
Qureshi AM, Justino H, Heinle JS. Transposition of the Great Arteries. In: Shaddy R, Penny D, Feltes T, Cetta F, Mital S. Moss & Adams heart disease in infants, children, and adolescents: Including the fetus and young adult. 10th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2022: 1122-1142.
Ahlström L, Odermarsky M, Malm T, Johansson Ramgren J, Liuba P. Preoperative coronary anatomy assessment with echocardiography and morbidity after arterial switch operation of transposition of the great arteries. Pediatr Cardiol. 2018;39(8):1620-1626. doi:10.1007/s00246-018-1939-z
