Authors: M.Gangadharan, MD, FAAP, FASA Children’s Memorial Hermann Hospital, University of Texas Health Science Center, Houston, TX AND K.L. Richards, MD, Children’s Hospital of Los Angeles, Univ. of Southern California, Keck School of Medicine, Los Angeles, CA
The echocardiogram of a newborn boy with clinical features of Trisomy 21 reveals a complete atrioventricular septal defect. The superior bridging leaflet of the atrioventricular valve has no chordal attachments to either ventricle. According to the Rastelli classification, what type of morphology BEST describes this atrioventricular valve?
EXPLANATION
Atrioventricular septal defects (AVSD) occur at a frequency of 2 per 10,000 live births and constitute about 3% of cardiac malformations. The defect is characterized by the combination of an ostium primum atrial septal defect (ASD), an inlet ventricular septal defect (VSD), and an abnormal atrioventricular valve (AVV) straddling the left and right chambers of the heart. It results from the failure of endocardial cushions to fuse in the fifth week of intrauterine development. The abnormal atrioventricular valve usually has five leaflets: the superior bridging leaflet (SBL), the inferior bridging leaflet (IBL), the right mural leaflet, the right antero-superior leaflet, and the left mural leaflet. The valve may have a single orifice, or two orifices as shown in Figure 1 below.
The pattern of the chordal septal attachments of the superior bridging leaflet (SBL) described by Rastelli is used to classify the morphology of the common atrioventricular valve into three subtypes. Rastelli type A, the most common subtype occurring in 75% of cases, consists of a superior bridging leaflet which is attached to the left ventricular septum through multiple chordal attachments. The AVV in type A is divided at the septum into left and right components. Rastelli type B, the rarest subtype, is characterized by a large SBL that extends across the interventricular septum and is attached to the right ventricle through an anomalous papillary muscle. The Rastelli type C atrioventricular valve consists of a very large SBL which is “free-floating” and unattached. The Rastelli classification may be used to determine the type of approach through either a one-patch or a two-patch technique.
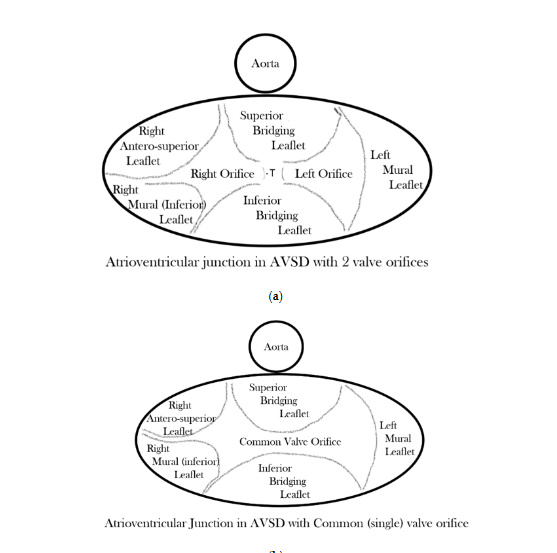
Figure 1. AVSD. (Rigby M. Atrioventricular Septal Defect: What Is in a Name?. J Cardiovasc Dev Dis. 2021;8(2):19. Distributed under Creative Commons Attribution License )
In addition to complete atrioventricular septal defect, there are also partial and transitional atrioventricular septal defects. Partial AVSDs consist of an ostium primum ASD and a gap at the zone of apposition between the left side of the SBL and IBL, which is often called a cleft. Transitional AVSDs consist of an ostium primum ASD, a restrictive VSD below the common atrioventricular valve, and a cleft.
Several cardiac malformations may occur with AVSD such as left ventricular inflow tract and outflow tract obstruction, tetralogy of Fallot, persistent left superior vena cava, coarctation of aorta, and heterotaxy. The common atrioventricular valve may open predominantly into the left or right ventricle resulting in an unbalanced AVSD and single ventricle physiology. Rastelli type A is associated with a narrow left ventricular outflow tract, often described as a “gooseneck deformity.” Rastelli type C is associated with tetralogy of Fallot. Complete diagnosis in the newborn period is usually possible with transthoracic echocardiography.
Multiple chromosomal anomalies have been associated with complete atrioventricular septal defects. It occurs in approximately 20% of infants and children with Trisomy 21 and is also commonly associated with tetralogy of Fallot. Complete AVSD occurs in almost all patients with asplenia and 25% of patients with polysplenia. In addition, 8p deletion syndrome, Trisomy 9, and Trisomy 18 are also associated with CAVSD.
The superior bridging leaflet of the atrioventricular valve described in the stem has no attachments, which describes the Rastelli type C morphology, unlike Rastelli type A and B.
REFERENCES
Walker SG. Anesthesia for Left-to-Right Shunt Lesions. In: Andropoulos DB, Mossad EB, Gottlieb EA. Anesthesia for Congenital Heart Disease. 4th Edition. Hoboken, NJ: John Wiley & Sons Ltd, Blackwell Publishing; 2023:636-637.
Rigby M. Atrioventricular Septal Defect: What Is in a Name? J Cardiovasc Dev Dis. 2021;8(2):19. doi:10.3390/jcdd8020019
Calabrò R, Limongelli G. Complete atrioventricular canal. Orphanet J Rare Dis. 2006;1:8. doi:10.1186/1750-1172-1-8
Marino B, Vairo U, Corno A, et al. Atrioventricular canal in Down syndrome. Prevalence of associated cardiac malformations compared with patients without Down syndrome. Am J Dis Child. 1990;144(10):1120-1122. doi:10.1001/archpedi.1990.02150340066025
