Author: Nicholas Houska, DO - University of Colorado - Children’s Hospital Colorado
A six-day-old boy with a prenatal diagnosis of D-transposition of the great arteries and ventricular septal defect presents for arterial switch operation and ventricular septal defect repair. Which of the following Society of Thoracic Surgeons and the European Association for Cardio-thoracic Surgery Congenital Heart Surgery Mortality Categories characterize this surgical procedure?
EXPLANATION
Given the complexity and heterogeneity of congenital heart disease and surgical repair, comparison of procedures proves challenging when analyzing outcomes and data. Historically, procedure risk and complexity were categorized using methodologies based on expert opinion such as the Aristotle Basic Complexity Score (ABC Score) and ABC Level (ABC Level), in addition to the Risk Adjustment for Congenital Heart Surgery-1 (RACHS-1) methodology. With the creation of large databases of surgical outcomes, it became apparent that a more quantitative and validated scoring system was needed in recent decades.
In 2009 O’Brien et al. analyzed the mortality risk of 148 types of operations that had been conducted on more than 77,000 patients who were entered into the European Association for Cardiothoracic Surgery (EACTS) Congenital Heart Surgery database and the Society of Thoracic Surgeons (STS) Congenital Heart Surgery database. Procedure-specific mortality rate estimates were calculated, and each procedure was assigned a numeric score, ranging from 0.1 to 5.0 based on the estimated mortality rate. This score was termed the STS-EACTS Congenital Heart Surgery Mortality Score or STS-EACTS score, more commonly referred to as STAT mortality categories. These surgical procedures were then grouped into five categories, referred to as the STS-EACTS Congenital Heart Surgery Mortality Categories (STS-EACTS categories). This scoring system categorizes procedures based on complexity and mortality, with category 1 being the lowest mortality risk and category 5 being the highest mortality risk. This model was then independently validated and compared with the ABC Score and the RACHS-1 score. The STS-EACTS scores and categories have demonstrated high discrimination (C-index) for predicting mortality as compared to the prior models. Although there are numerous congenital cardiac diagnoses for specific surgical procedures, representative examples of procedures and mortality categories are shown in Table 1 below.
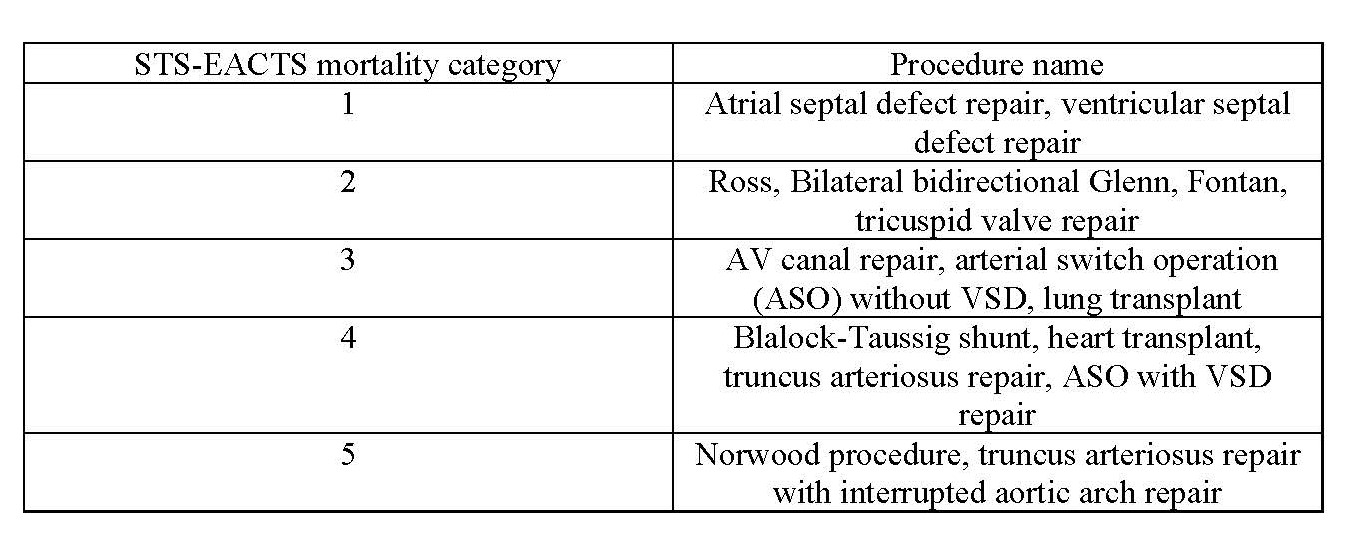 Table 1: Common examples of procedures in each STS-EACTS mortality category.
Table 1: Common examples of procedures in each STS-EACTS mortality category.
The STS-EACTS mortality categories have been increasingly utilized for both research and outcomes reporting. They are utilized in the STS Congenital Heart Surgery Database public reporting of mortality risk for participating hospitals. Given the expanded availability of this data, patients and parents are increasingly aware of and utilize this information when choosing a hospital for surgical care of congenital heart disease.
REFERENCES
O'Brien SM, Clarke DR, Jacobs JP et al. An empirically based tool for analyzing mortality associated with congenital heart surgery. J Thorac Cardiovasc Surg. 2009;138(5):1139-53. doi: 10.1016/j.jtcvs.2009.03.071. PMID: 19837218.
Jacobs JP, Jacobs ML, Maruszewski B et al. Initial application in the EACTS and STS Congenital Heart Surgery Databases of an empirically derived methodology of complexity adjustment to evaluate surgical case mix and results. Eur J Cardiothorac Surg. 2012;42(5):775-779 i: 10.1093/ejcts/ezs026.
Jacobs JP, Jacobs ML, Lacour-Gayet FG et al. Stratification of complexity improves the utility and accuracy of outcomes analysis in a Multi-Institutional Congenital Heart Surgery Database: Application of the Risk Adjustment in Congenital Heart Surgery (RACHS-1) and Aristotle Systems in the Society of Thoracic Surgeons (STS) Congenital Heart Surgery Database. Pediatr Cardiol. 2009;30(8):1117-1130. doi: 10.1007/s00246-009-9496-0. PMID: 19771463.
The Society for Thoracic Surgeons Public Reporting. https://publicreporting.sts.org/chsd. Accessed November 13, 2024.