Author: Kaitlin M. Flannery, MD, MPH - Stanford University
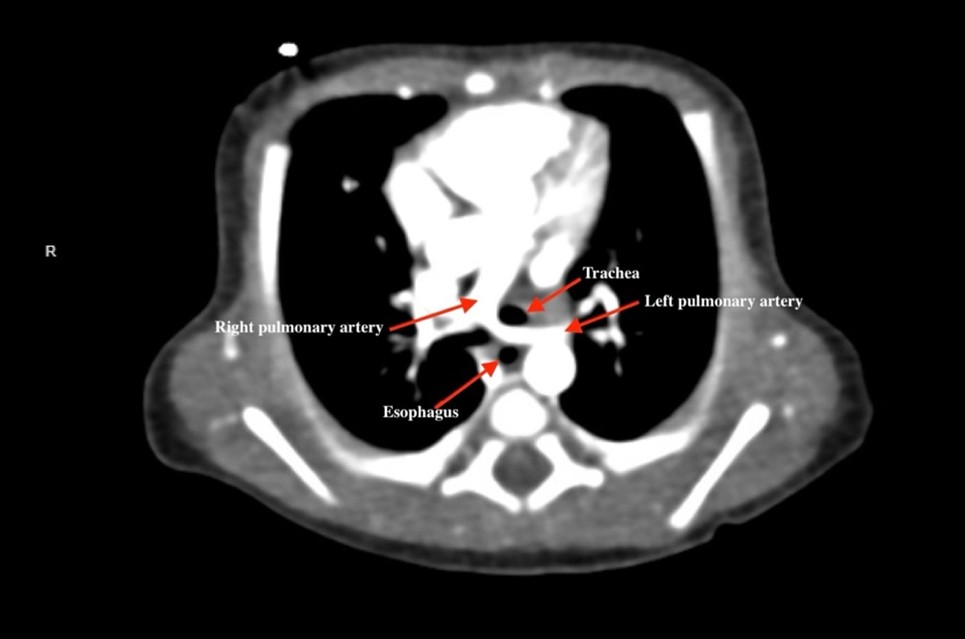
A 2-day-old, 3.1kg, term neonate has required non-invasive positive pressure ventilation and oxygen administration since delivery due to increased work of breathing and low oxygen saturation. A transthoracic echocardiogram was performed and subsequently a CT scan of the chest with contrast. An image from the CT is displayed. What is the diagnosis?
EXPLANATION
Vascular rings are congenital malformations that result from abnormal embryologic development and regression of the ventral and dorsal aortae and the six paired pharyngeal arches. The malformation results in an encircling and possible compression of the trachea and esophagus. Some present with severe symptoms at birth while others are incidentally found.1
The Society of Thoracic Surgeons (STS) utilizes the Backer and Mavroudis classifications system. This system divides vascular rings into four categories. These categories account for about 95% of pathology seen. The categories with incidence are:2
1. Double Aortic Arch (0.53%) – presence of both left and right-sided aortic arches encircling the trachea and esophagus
2. Right aortic arch with left ligamentum (0.05%) – presence of aberrant right-sided aortic arch with left ligamentum arteriosum attached to left subclavian artery or descending aorta, encircling the trachea and esophagus
3. Innominate artery compression syndrome (0.004%) – not a true vascular ring; occurs mostly when innominate artery origin is more distal or posterior, thus passing across the front of the trachea
4. Pulmonary artery sling (0.006%) – not a true vascular ring; aberrant origin of one pulmonary artery arising from the other; passes between the trachea and esophagus at a level close to the carina4
The CT shows the left pulmonary artery arising from the right pulmonary artery and coursing between the trachea and esophagus thereby creating a pulmonary artery sling (PAS). Patients with PAS typically present after a few months of life with significant respiratory symptoms as the disease is associated with tracheal stenosis from complete tracheal rings.1 The severity of symptoms and management depend on the degree and length of tracheobronchial narrowing. The largest case series on surgical management of PAS was published in 2012.3 The series reports the outcomes of 34 patients repaired on CPB from 1985-2012. The surgical approach to tracheal repair changed over the years with slide tracheoplasty utilized since 2002. Slide tracheoplasty is mostly used in cases of long-segment stenosis, and consists in transection and oblique division of the proximal and distal trachea, with subsequent anastomosis of each end, thereby increasing lumen size. Short segment stenosis may be managed with excision of diseased segment and end-to-end anastomosis. The aberrant pulmonary artery is often reimplanted during the same surgery. In this series, 79% of patients had tracheal stenosis from complete tracheal rings. There were no early deaths in this series. The mean percent of LPA blood flow was 41% with only one patient requiring reintervention for stenosis. There were four late deaths in this series, two were unrelated PAS, and two were due to complications from older surgical techniques for complete tracheal rings that resulted in dehiscence during follow-up bronchoscopy.3
REFERENCES
1. Ragalie WS, Mitchell ME. Chapter 44: Vascular rings and pulmonary artery slings. In: Ungerleider RM, Meliones JN, McMillan KN, Cooper DS, Jacobs JP, eds. Critical Heart Disease in Infants and Children. 3rd ed. Elsevier; 2019: 544-50.
2. Wadle M, Joffe D, Backer C, Ross F. Perioperative and anesthetic considerations in vascular rings and slings. Semin Cardiothorac Vasc Anesth. 2024 Sep;28(3):152-64.
3. Backer CL, Russel HM, Kaushal S, et al. Pulmonary artery sling: current results with cardiopulmonary bypass. J Thorac Cardiovasc Surg. 2012 Jan;143(1):144-51.
4. McKenzie I, Zestos MM, Stayer SA, Kaminski E, Davies P, Andropoulos DB. Anesthesia for miscellaneous cardiac lesions. In: Andropoulos DB, Mossad EB, Gottlieb EA. Eds. Anesthesia for Congenital Heart Disease. 4th Ed. Wiley Blackwell; 2023:781-831.
