Authors: Philicia Findlay-Hardyal, MD and Arturo Marrero, MD- Georgetown Public Health Corporation - Georgetown, Guyana AND Destiny F. Chau, MD - Arkansas Children’s Hospital/University of Arkansas for Medical Sciences, Little Rock, AR, USA
A 3-month-old infant with a suspected vascular ring is undergoing rigid bronchoscopy, which demonstrates the presence of complete tracheal rings. Which of the following types of vascular rings is MOST likely present in this patient?
EXPLANATION
Vascular rings describe congenital anomalies whereby the aortic arch and its primary branches form a circle around the trachea, the esophagus, or both, potentially resulting in tracheal and/or esophageal obstruction and obstructive symptoms. The incidence of isolated vascular rings has been reported as seven in 10,000 live births (0.07%). As vascular rings are rare, diagnosis requires a high index of clinical suspicion. Patients may be misdiagnosed with refractory asthma and/or gastrointestinal pathology, thus deferring further workup until the vascular ring is finally diagnosed.
The embryologic mechanism for vascular rings originates from the interruption at different stages of the normal regression of the six pharyngeal arches that are connected to the dorsal aortae during the embryologic development of the aortic arch and its main branches. This results in the persistence of vascular structures or ligamentous remnants that may compress the trachea or esophagus.
The majority of vascular ring malformations can be classified into the following grouping system described by Backer and Mavroudis:
A. Double aortic arch: the left and right aortic arches encircle the trachea and esophagus.
B. Right aortic arch with left ligamentum: the aortic arch is to the right of the trachea, with the ligamentum connecting the main pulmonary artery to the descending aorta.
C. Innominate artery compression syndrome: the innominate artery compresses the anterior trachea by over 80%.
D. Pulmonary artery sling: the left pulmonary artery originates from the right pulmonary artery traveling posteriorly, between the trachea and esophagus.
The figure below illustrates reconstructed computed tomography of the different types of vascular rings.
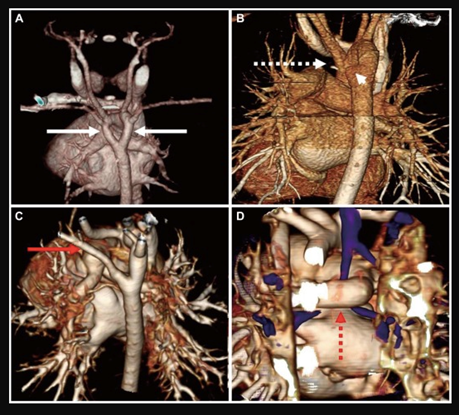 Figure: Vascular rings reconstructed from cardiac computed tomography. A: double aortic arch; two aortic arches (white bold arrows) comprise the complete ring in this patient. B: right aortic arch with persistent left ligamentum arteriosum; Kommerell's diverticulum (arrowhead) and fibrotic band (white dotted arrows) comprise the complete ring in this patient. C: right aortic arch with aberrant left subclavian artery (red bold arrow). D: pulmonary sling; left pulmonary artery originates from the right pulmonary artery (red dotted arrow), compressing the bronchus.
Source: Suh YJ, Kim GB, Kwon BS, et al. The clinical course of vascular rings and risk factors associated with mortality. Korean Circ J. 2012;42(4):252-258. doi:10.4070/kcj.2012.42.4.252- Creative Commons License
Figure: Vascular rings reconstructed from cardiac computed tomography. A: double aortic arch; two aortic arches (white bold arrows) comprise the complete ring in this patient. B: right aortic arch with persistent left ligamentum arteriosum; Kommerell's diverticulum (arrowhead) and fibrotic band (white dotted arrows) comprise the complete ring in this patient. C: right aortic arch with aberrant left subclavian artery (red bold arrow). D: pulmonary sling; left pulmonary artery originates from the right pulmonary artery (red dotted arrow), compressing the bronchus.
Source: Suh YJ, Kim GB, Kwon BS, et al. The clinical course of vascular rings and risk factors associated with mortality. Korean Circ J. 2012;42(4):252-258. doi:10.4070/kcj.2012.42.4.252- Creative Commons License
Once clinical suspicion arises, confirmatory diagnosis is usually made by cardiac computed tomography or magnetic resonance imaging. Echocardiography is unreliable for definitive diagnosis but does aid in the detection of associated cardiac anomalies occurring in approximately 12% of patients. Bronchoscopy allows for the delineation of tracheal abnormalities, such as tracheobronchomalacia, and for the detection of complete tracheal rings.
Except for pulmonary artery slings, vascular ring repair is usually performed through a thoracotomy for surgical division of the ring. Surgical repair of a pulmonary artery sling is performed through a median sternotomy approach and under cardiopulmonary bypass, as the left pulmonary artery needs to be translocated. Additionally, 60-80% of patients with pulmonary artery slings also have tracheal stenosis secondary to complete cartilaginous tracheal rings, which are repaired during the same procedure. Tracheal reconstruction is usually recommended after the vascular ring repair to avoid contamination of the surgical field from secretions within the trachea. The most common repair for complete tracheal rings is a slide tracheoplasty for long-segment stenosis. Resection of a short, narrowed segment of complete tracheal rings may be repaired with an end-to-end anastomosis. Although survival rates are excellent, patients often require repeat airway evaluation and intervention for persistent tracheomalacia, granuloma formation, or balloon dilation. Patients also require regular follow-up to evaluate for the development of left pulmonary artery stenosis.
In this infant, the presence of the complete tracheal rings indicates a moderate to high probability of a pulmonary artery sling. Although double aortic arch and right aortic arch/left ligamentum are much more common than pulmonary artery slings, they are not typically associated with complete tracheal rings.
REFERENCES
Wadle M, Joffe D, Backer C, Ross F. Perioperative and anesthetic considerations in vascular rings and slings. Semin Cardiothorac Vasc Anesth. 2024;28(3):152-164. doi:10.1177/10892532241234404
Worhunsky DJ, Levy BE, Stephens EH, Backer CL. Vascular rings. Semin Pediatr Surg. 2021;30(6):151128. doi:10.1016/j.sempedsurg.2021.151128
McKenzie I, Markakis Zestos M, Stayer S, Kaminski E, Davies P, Andropoulos D. Anesthesia for miscellaneous lesions. In: Andropoulos D, Mossad E, Gottlieb E, eds. Anesthesia for Congenital Heart Disease. 4th Edition. New Jersey: John Wiley & Sons, Inc.; 2023: 816-820.
Suh YJ, Kim GB, Kwon BS, et al. Clinical course of vascular rings and risk factors associated with mortality. Korean Circ J. 2012;42(4):252-258. doi:10.4070/kcj.2012.42.4.252