Author: Anila B. Elliott, MD, University of Michigan - C.S. Mott Children’s Hospital
A 3-year-old girl is undergoing surgical repair of an atrial septal defect via median sternotomy. A deep parasternal intercostal plane (DPIP) block is performed at the end of the procedure to facilitate early extubation and post-operative analgesia. Which of the following nerves are the primary targets of this block?
EXPLANATION
Effective management of perioperative pain in pediatric cardiac surgery is important, as inadequate pain control has been linked to a range of complications, including extended ICU and hospital stays, respiratory complications, prolonged intubation and hemodynamic instability.1 Regional anesthesia is increasingly being utilized as a key component of a multimodal approach to improve the perioperative care of this patient population.2 Due to the increasing numbers of regional techniques that are being described, there is significant heterogeneity and confusion about nomenclature. El-Boghdadly et al. attempted to standardize the nomenclature to improve communication, education and training.5
One current technique is the deep parasternal intercostal plane block (DPIP) (formerly termed transversus thoracic muscle plane (TTMP) block), which was first described in 2015 by Ueshima and colleagues.3 It has been shown to be effective in providing analgesia for surgeries involving a median sternotomy. This muscle plane block involves injecting local anesthetic bilaterally, between the transversus thoracic muscle and the internal intercostal muscles. It targets the anterior cutaneous branches of the intercostal nerves (T2-T6) to provide analgesia to the anterior chest wall.4
Although many studies of the efficacy of this regional technique have been performed on adult patients, there are a select few that have investigated the impact on pediatric cardiac surgery patients.4 The DPIP block offers several advantages, including a reduction in opioid consumption, decreased pain scores, improved hemodynamic stability and enhanced recovery following open-heart surgery.2,4 Complications of the block include vascular injury to nearby vasculature, hematoma, infection, and pneumothorax.4
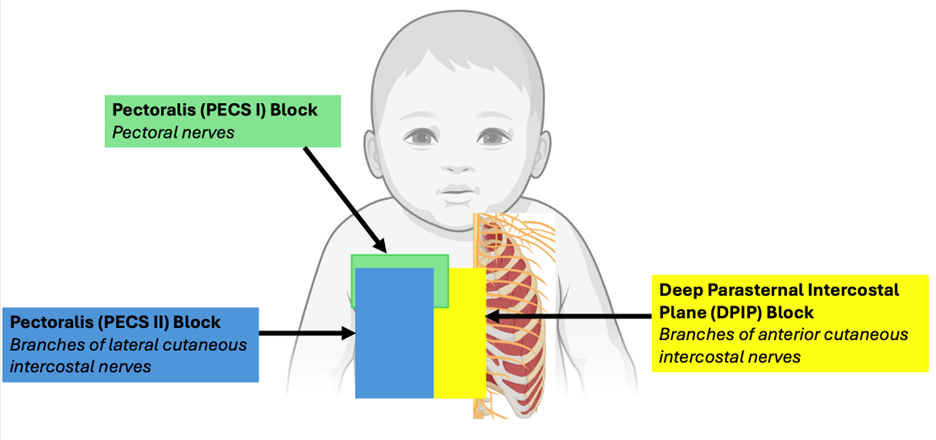
There are other regional anesthetic techniques for the anterior chest wall that can be performed as part of surgery involving a median sternotomy. The superficial parasternal intercostal plane block (SPIP), formerly termed the pecto-intercostal fascial plane block (PIFB), also blocks the anterior cutaneous branches of the intercostal nerves, and is thought to have a superior safety profile when compared to the deep version of the block, especially in children. Pectoralis blocks (PECS I and PECS II) can also be performed for sternal analgesia.5 The PECS I block targets the pectoral nerves, whereas the PECS II block targets the lateral branches of the intercostal nerves (T2-T6).4
Figure 1: Summary of innervation of regional blocks for procedures on the anterior chest wall
Additionally, the erector spinae plane (ESP) block has been shown to be effective in pediatric cardiac surgery. This block targets the dorsal and ventral rami of the thoracic and abdominal spinal nerves, providing reliable coverage of the posterior chest wall.4 However, studies have found that its analgesic effect on the anterior chest wall can be inconsistent.
As regional anesthetic techniques continue to evolve, it is important for congenital cardiac anesthesiologists to stay informed about these advancements to optimize patient care and recovery. In this patient, the planned DPIP block would target the anterior cutaneous branches of the intercostal nerves, which is answer B. The lateral cutaneous branches are primarily targeted by posterior chest wall regional techniques, and the pectoral nerves are blocked by the two pectoralis blocks.
REFERENCES
1. Aydin, ME., Ahiskalioglu, A., Ates, I., et al. Efficacy of ultrasound-guided transversus thoracic muscle plane block on postoperative opioid consumption after cardiac surgery: a prospective, randomized, double-blind study. JCVA 2020; 34(11): 2996-3003
2. Cakmak, M., Isik, O. Transversus thoracic muscle plane block for analgesia after pediatric cardiac surgery. JCVA 2021; 35(1): 130-136
3. Ueshima, H., Kitamura, A. Clinical experiences of ultrasound-guided transversus thoracic muscle plane block: a clinical experience. J Clin Anesth 2015; 27: 428-429
4. Dost, B., De Cassai, A., Amaral, S., et al. Regional anesthesia for pediatric cardiac surgery: a review. BMC Anesthesiology 2025; Retrieved at: https://bmcanesthesiol.biomedcentral.com/articles/10.1186/s12871-025-02960-z#ref-CR1
5. El-Boghdadly K, Wolmarans M, Stengel AD, et al. Standardizing nomenclature in regional anesthesia: an ASRA-ESRA Delphi consensus study of abdominal wall, paraspinal, and chest wall blocks. Reg Anesth Pain Med. 2021;46(7):571-580. doi:10.1136/rapm-2020-102451